Dietary Fiber Benefits: What It Is, How It Works, and Why It Matters for Metabolism, Gut Health, and Prevention
- Pubblicazione 30/06/2026
- Aggiornamento 30/06/2026
- Revisione 30/06/2026
- Storia articolo

IN BRIEF: WHAT THE SCIENCE SAYS
Dietary Fiber: What Is It, and Why Is It So Important Today?
In brief: Dietary fiber consists of plant components that influence the gut, blood glucose, satiety, and lipid profile. It has become central because it helps reveal the true quality of a diet and its effects on metabolism.

When people talk about dietary fiber, many still associate it almost exclusively with bowel regularity. That view is now too narrow compared with what the evidence actually shows. Fiber is a broad and highly heterogeneous family of compounds found mainly in legumes, whole grains, vegetables, fruit, seeds, and nuts. Its current scientific relevance comes from the fact that it interacts with a wide range of physiological processes that extend far beyond simple intestinal transit. Available data show that its role includes meal dynamics, the rate of nutrient absorption, modulation of LDL cholesterol, that is, the low-density lipoprotein involved in cholesterol transport in the blood, and the production of biologically active intestinal metabolites [2][14].
This growing importance also reflects changes in the modern food environment. Contemporary diets tend to favor more refined and less structurally complex products, with a marked reduction in dietary fiber intake and, as a result, in the functional complexity of meals. In this setting, talking about fiber also means talking about carbohydrate quality, the structural density of foods, and the way the body manages energy, hunger, satiety, and its relationship with the gut microbiota, that is, the community of bacteria, archaea, and other microorganisms living in the large intestine and involved in numerous metabolic functions [3][17].
Another crucial point is that fibers do not all behave in the same way. Some hold water and form gels, some increase stool bulk, and others are fermented and generate short-chain fatty acids, molecules produced through bacterial activity that take part in the dialogue between the gut and metabolism. The evidence makes it clear that this heterogeneity prevents fiber from being treated as a single nutrient with a single effect. Instead, it requires distinctions based on properties, use context, and practical implications. A few foundational concepts are especially useful here:
- Dietary fibers are not all the same, and their function changes according to their structure.
- Solubility, viscosity, and fermentability lead to different physiological effects.
- Daily intake matters because benefits emerge through continuity, not occasional use.
- The modern diet tends to provide too little fiber, especially when refined products dominate.
- Individual tolerance varies, so a gradual increase is often necessary, particularly when baseline intake is low.
What dietary fiber really is
Dietary fiber consists of plant components that resist digestion and absorption in the small intestine to varying degrees and reach the colon, where they may be fermented by intestinal bacteria or eliminated largely unchanged. That definition is accurate, but it remains incomplete unless it is clear that the physiological behavior of fiber depends on specific properties such as solubility, viscosity, fermentability, and molecular structure, that is, the chemical organization that shapes its interaction with water, nutrients, and the microbiota. The evidence shows that this diversity leads to different effects on blood glucose, lipid profile, and the perception of satiety, which is why it is misleading to treat fiber as a single nutrient with a uniform effect [3]. From a biological perspective, some fibers slow gastric emptying, some interfere with glucose diffusion in the intestinal lumen, and others serve as a preferred substrate for bacterial fermentation. In other words, the term fiber does not describe one simple entity, but a family of compounds with complementary and partly overlapping roles. Available data also suggest that the benefits seen in epidemiological studies are linked in part to the fact that fiber often comes with a dietary pattern richer in minimally refined plant foods and therefore with a more favorable overall diet quality [2][17]. Recognizing this heterogeneity helps avoid practical oversimplifications, such as the idea that simply “eating more fiber” is enough without considering source, type, and context. What matters in practice is the way fiber changes the physiology of the meal and its downstream impact on the relationship between the gut and metabolism. From here, the most familiar next step is the classic distinction between soluble and insoluble forms.
Soluble and insoluble fiber: what really changes
The distinction between soluble fiber and insoluble fiber is the one most commonly used in nutrition communication. Still, it should be seen as a first point of orientation rather than a complete explanation of all the physiological effects observed. Soluble fibers disperse in water and, in some cases, form viscous solutions or gels that alter digestive dynamics by slowing gastric emptying and reducing the speed at which nutrients reach the absorptive surface of the intestine. This helps explain why some of these fibers are associated with a more gradual glycemic response and favorable effects on LDL cholesterol [5]. Insoluble fibers, by contrast, tend to have a more visible effect on stool bulk and intestinal transit, making them especially relevant for bowel regularity and for the prevention of constipation, the medical term for persistent difficulty with bowel evacuation or a reduced frequency of bowel movements. Even so, this distinction remains incomplete if used as the only framework, because some soluble fibers are not especially viscous, while some insoluble fibers can exert effects that go beyond simply increasing stool volume [8]. Meta-analyses show that clinical outcomes often depend more on functional properties, such as the ability to form gels or to undergo fermentation, than on the simple label “soluble” or “insoluble” [5]. In other words, the classification is useful for introducing the topic, but it is not enough to meaningfully guide nutritional practice. To understand why one type of fiber may be more active than another, it is necessary to look at fermentability, which directly links fiber, intestinal bacteria, and active metabolites.
Fermentable and non-fermentable fiber
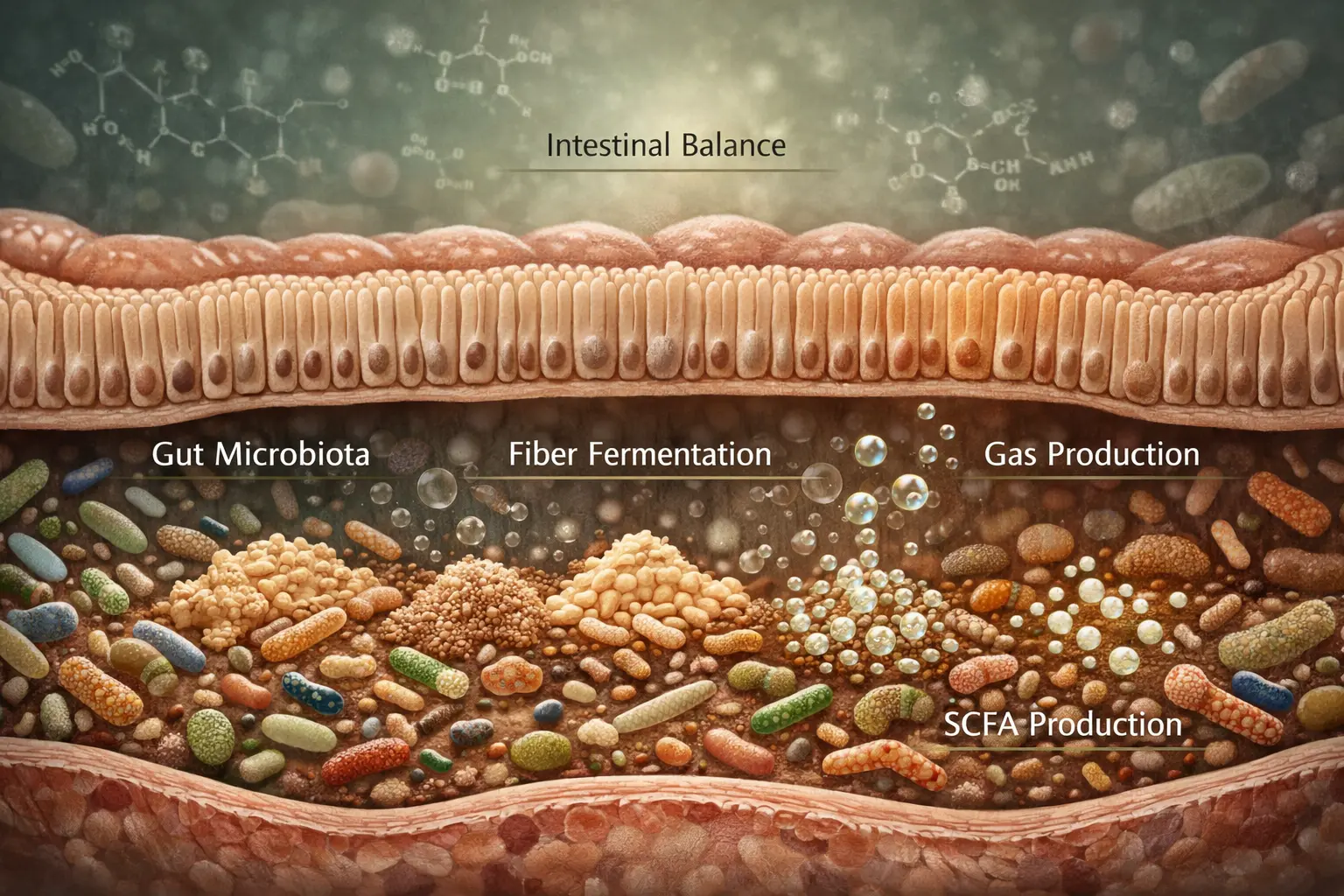
A distinction that more closely reflects real physiology is the one between fermentable fiber and non-fermentable fiber, because it brings the role of the gut microbiota and its metabolic products into focus. Fermentable fibers are used by colon bacteria as an energy substrate, and this process gives rise to SCFAs, that is, short-chain fatty acids such as acetate, propionate, and butyrate. These molecules are not passive byproducts. They help maintain the intestinal barrier, support the energy needs of colon cells, and modulate signals that connect the gut, metabolism, and inflammation [10][11]. Non-fermentable fibers, in contrast, mainly exert mechanical effects by increasing stool bulk and facilitating intestinal transit. That does not make them less important, but it does clarify their primary role. The evidence indicates that the response to fermentation is not the same in every individual, because the starting composition of the microbiota has a major influence on both the capacity to produce metabolites and the way the gut tolerates higher fiber intake [9][10]. This individual variability helps explain why increasing fiber feels beneficial for some people yet initially uncomfortable for others, especially when bloating or gas production is involved. In this context, talking about fermentable fiber means talking about a dynamic interaction among food, bacteria, and host physiology. That naturally leads to the issue of viscosity, which adds another layer of understanding to the metabolic effects of fiber.
Viscous and non-viscous fiber
Viscosity is a key property of fiber. It is often less familiar to the general public, yet it is highly relevant in clinical terms because it affects the consistency of digestive contents and, as a result, the speed at which nutrients and bile molecules move through the intestinal lumen. Viscous fibers form gels or dense solutions that slow glucose diffusion, modulate gastric emptying, and help make the metabolic response after a meal less abrupt. Meta-analyses show that these fibers can reduce postprandial blood glucose and improve some parameters of glycemic control in individuals with type 2 diabetes, a condition characterized by altered glycemic regulation and insulin resistance [5][6]. Viscosity also matters in lipid metabolism, because some viscous fibers interfere with bile acid reabsorption and promote greater use of cholesterol for bile acid resynthesis, thereby contributing to lower LDL cholesterol. Non-viscous fibers may still be useful, but they generally have less pronounced effects on these specific outcomes. This makes it clear why the practical recommendation cannot be reduced to a generic “increase fiber,” but must instead take into account the functional profile of the fiber being consumed [6][17]. In other words, fiber should not be assessed only by quantity, but by how it behaves during digestive transit. Understanding viscosity allows for a more precise reading of the relationship between fiber, blood glucose, satiety, and lipids. At this stage, the next logical question is daily intake, because even the most interesting fiber has limited impact if total consumption remains too low.
How much fiber should you consume each day?
The question of how much dietary fiber to consume each day is one of the most common, but the answer requires an important distinction between the minimum recommended threshold and the amount that is truly adequate for the individual. International guidelines often point to a reference value of around 25 grams per day for adults, while several recommendations suggest higher amounts depending on energy intake and clinical context. The evidence shows a dose-response relationship between higher fiber intake and lower risk of chronic disease, with clear benefits especially at intakes of around 25–29 grams per day or more [3][14]. That said, this threshold should not be treated as a magic number or as the same target for everyone, because real-world needs depend on age, calorie intake, diet quality, intestinal tolerance, metabolic status, and the presence of digestive symptoms. Many people start from much lower intakes, so even gradual increases can lead to noticeable improvements without requiring drastic changes. By contrast, a sudden increase, especially in people who consume little fluid or have intestinal sensitivity, can worsen bloating and discomfort [8]. So the issue is not only reaching a certain threshold, but gradually building a sustainable pattern that fits the individual context. This leads directly to another key question: if the recommendations are well known, why does the modern diet still remain so low in fiber?
Why fiber is missing from the modern diet
The low fiber content of the modern diet does not stem from one single poor choice, but from a broader transformation in the way food is produced, purchased, and consumed. Greater reliance on refined and highly processed foods sharply reduces fiber content, but it also alters meal structure, the rate of carbohydrate digestion, and the overall satiating quality of the diet. When a grain is refined, for example, the loss is not limited to one fraction of fiber. The entire plant matrix that helped slow nutrient absorption and shape digestive physiology is altered [3][16]. This trend is reinforced by lower consumption of legumes, vegetables, whole fruit, and whole grains, that is, the main natural sources of fiber, with a resulting decrease in the variety of substrates available to the gut microbiota. Prospective evidence indicates that dietary patterns richer in fiber and plant foods are associated with lower risk of chronic disease and mortality, but this finding should be interpreted as part of an overall dietary pattern rather than as the isolated effect of a single nutrient [14][16]. The real issue, then, is not simply that people consume too little fiber today. It is that they are eating fewer structurally complex foods and more convenient products with low functional density. This closes the first major section and sets the stage for the next one, where the focus shifts to how fiber actually works in the body after a meal.
How Fiber Works in the Body: From Meals to Metabolism
In brief: Fiber changes the way the body handles a meal by slowing absorption, influencing lipids, and nourishing the microbiota. That is why it has a concrete impact on blood glucose, satiety, and metabolic profile.
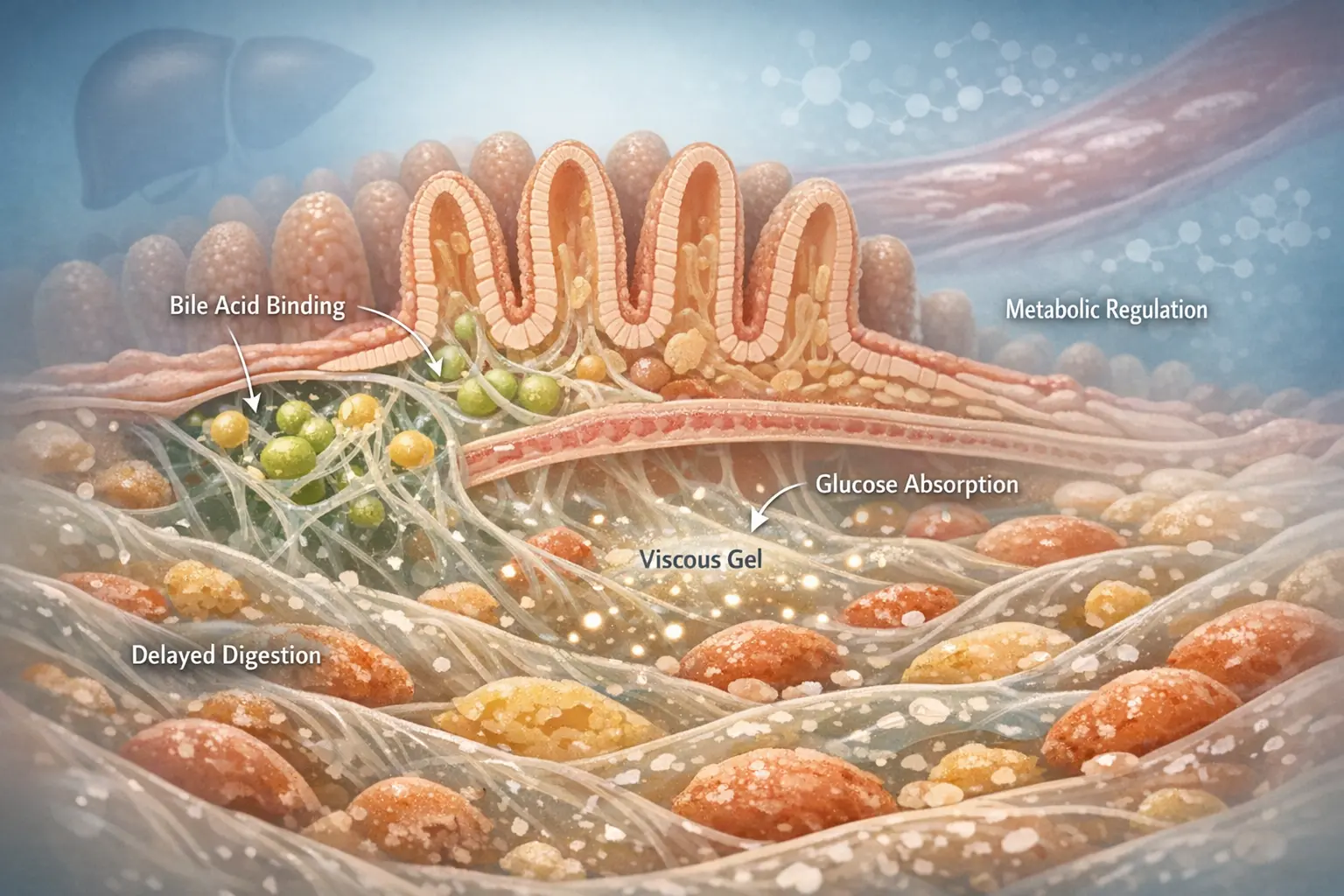
Once it is clear what dietary fiber is, the next step is to understand how it works in the body, because its real value becomes most evident when we look at the way it changes meal physiology. Fiber does not exert its effects simply because it “is not digested,” but because it changes the behavior of food contents throughout the gastrointestinal tract, alters the consistency of the bolus and chyme, slows or modulates the interaction between nutrients and the intestinal mucosa, and, in many cases, enters into dialogue with the gut microbiota, which in turn produces metabolites involved in metabolic regulation [10][17]. Its action is therefore best understood as a sequence of connected steps. In the stomach, some fibers increase the volume and density of contents, contributing to greater stomach distension and slower gastric emptying. In the small intestine, viscous fibers can make the diffusion of glucose and lipids toward the absorptive surface more gradual, influencing postprandial blood glucose, that is, the rise in blood glucose after a meal, as well as the dynamics of insulin response. In the colon, fermentable fibers become a substrate for bacteria, generating compounds such as butyrate, acetate, and propionate, which participate in both local and systemic functions [6][11]. Available evidence shows that higher fiber intake is associated with improvements in major cardiometabolic risk factors, although the size of these effects varies according to fiber type, dose, and overall dietary context [17]. This point is crucial, because it prevents fiber from being treated as though it had an automatic effect independent of the rest of the diet. More accurately, fiber should be viewed as an element that changes the physiological profile of the meal and, through that shift, influences several key points in metabolism. The main mechanisms can be summarized as follows:
- Fiber can slow nutrient absorption, especially when it is viscous.
- The insulin response changes indirectly because the speed at which glucose enters the bloodstream changes.
- Some fibers interfere with bile acid reabsorption, thereby influencing cholesterol metabolism.
- Fermentable fibers nourish the microbiota and promote the production of biologically active metabolites.
- The perception of satiety may increase because of greater volume, viscosity, and longer gastric retention.
How fiber affects glucose absorption
Dietary fiber, especially fiber with viscous properties, can reduce the rate at which glucose is absorbed after a meal. This effect depends mainly on two integrated mechanisms: slower gastric emptying and greater viscosity of intestinal contents, which slows the diffusion of glucose toward the mucosa of the small intestine. In practical terms, this means that blood glucose tends to rise more gradually, with less pronounced postprandial peaks than those seen after meals low in fiber or built around highly refined carbohydrates [5][6]. This point matters because the speed of glucose absorption does not affect only the value that may appear on a blood glucose check. It shapes the entire metabolic response to the meal. Meta-analyses on viscous fiber supplements show significant reductions in postprandial blood glucose and improvements in some markers of glycemic control in individuals with type 2 diabetes [6]. Even so, context remains essential, because fiber incorporated into a structured meal often has greater significance than an isolated fiber addition taken separately during the day. The available data therefore suggest that fiber does not “block” glucose, but changes the way glucose enters the bloodstream. This helps explain why meal quality matters more than an occasional add-on and naturally leads to the next issue: the resulting insulin response.
Fiber and postprandial insulin response
The postprandial insulin response depends largely on the rate at which glucose is absorbed and released into the bloodstream after a meal. For that reason, fiber can influence this response indirectly even without acting directly on insulin secretion, that is, the hormone produced by the pancreas that facilitates glucose entry into cells. When the rise in blood glucose is more gradual, the insulin response also tends to be less abrupt, and this may support more stable metabolic regulation over time, especially in individuals with impaired glucose tolerance [3][17]. Systematic reviews show that diets richer in fiber are associated with better glycemic and insulin parameters, particularly when the fiber comes from whole foods and from overall dietary patterns that are more favorable [3]. At the same time, oversimplification should be avoided, because the effect is not uniform across all studies and depends on factors such as fiber type, dose, overall carbohydrate quality, and the person’s metabolic status. Put simply, not all fibers improve insulin response in the same way, and not all individuals respond to the same extent. This confirms that the value of fiber does not lie in a single isolated action, but in its ability to modify the physiological context of the meal. Once that mechanism is clear, it becomes natural to turn to another extensively studied area: the relationship between fiber and LDL cholesterol, which introduces the role of bile acids.
Fiber and LDL cholesterol
One of the areas in which dietary fiber has been studied most extensively is LDL cholesterol, that is, the lipoprotein fraction that carries cholesterol from the liver to the tissues and that, when elevated over time, is associated with increased cardiovascular risk. Some fibers, particularly viscous ones, can interfere with bile acid reabsorption in the intestine, and this interaction is one of the main mechanisms through which fiber contributes to improvement in lipid profile [12][17]. When bile acids are excreted in greater amounts through the stool, the liver is forced to use more cholesterol to synthesize new bile acids. This does not eliminate the metabolic issue at its root, but it can help lower LDL levels in the blood, especially when increased fiber intake is part of a dietary pattern that is richer in plant foods and stronger in lipid quality overall. Meta-analyses indicate that fiber intake, especially from whole-food sources and from viscous fibers, is associated with improvements in lipid profile, although the overall magnitude of the effect remains moderate and context-dependent [4][17]. This point matters because it prevents exaggerated interpretations. Fiber is not a standalone shortcut for normalizing cholesterol, but a useful nutritional tool within a broader strategy. To understand this mechanism more fully, the next step is to focus directly on bile acids.
The role of bile acids
Bile acids are molecules synthesized by the liver from cholesterol and released into the intestine to facilitate fat digestion and absorption. Under normal conditions, a substantial portion of these molecules is reabsorbed in the intestine and returned to the liver through the so-called enterohepatic circulation, that is, the recycling system that allows bile acids to be reused multiple times. Some fibers, especially those with strong gel-forming capacity, can interfere with this process and reduce intestinal reabsorption, promoting greater fecal excretion [4][17]. This forces the body to use more cholesterol to synthesize new bile acids, creating one of the physiological mechanisms through which fiber contributes to lowering LDL cholesterol. The evidence summarized in systematic reviews indicates that this mechanism is biologically plausible and consistent with the improvements observed in lipid profile, although it does not produce identical effects in all individuals [4]. The response depends on the amount consumed, the consistency of intake, and the rest of the diet. In this context, the intestine no longer appears as a simple passageway for food, but as an active hub in metabolic regulation. And it is precisely this connection between the intestinal lumen, lipid metabolism, and systemic signaling that leads naturally to the role of the microbiota and short-chain fatty acids.
Fiber, the microbiota, and short-chain fatty acids
One of the most intensively studied areas in recent years is the relationship between dietary fiber, the gut microbiota, and the production of short-chain fatty acids, often referred to by the acronym SCFAs. When fermentable fibers reach the colon, they are metabolized by gut bacteria and produce compounds such as acetate, propionate, and butyrate. These molecules perform important biological functions: butyrate is a primary energy source for colon cells, while SCFAs as a whole help regulate the intestinal environment, the integrity of the mucosal barrier, and metabolic signaling pathways that also involve other organs [10][11]. Systematic reviews indicate that increasing fiber intake can alter microbiota composition and increase SCFA production, but they also show substantial variability between individuals and across studies, related to baseline microbiota composition, habitual diet, and differences in the type of fiber used [9][10]. For this reason, it is inaccurate to claim that fiber “normalizes” the microbiota in a uniform way. More accurately, fiber provides a substrate that may support a more active and diverse intestinal environment, but outcomes depend on the individual’s biological context. This complexity helps explain why fiber is involved simultaneously in digestive, metabolic, and immune functions, and clarifies that its effects do not stop within the gut. At this point, it is worth looking at another mechanism that is very noticeable in everyday life: its influence on satiety.
Fiber and satiety
Dietary fiber influences satiety through several integrated mechanisms that affect meal volume, gastric residence time, and the overall quality of the eating experience. First, many fibers increase food volume without proportionally increasing its energy content, contributing to greater gastric distension. Second, some fibers slow gastric emptying and prolong the feeling of fullness. In addition, foods that are naturally rich in fiber often require more chewing and are eaten more slowly, which may promote more conscious regulation of energy intake [7][19]. The evidence indicates that fiber supplementation, especially with soluble fiber, can increase perceived satiety and reduce energy intake, although the effects are generally modest and variable [19]. This suggests that fiber is not a direct or stand-alone weight-loss tool, but rather a useful support within a consistent dietary pattern built around minimally refined foods and a more favorable energy density. Its real contribution emerges above all when it improves meal quality and helps with appetite regulation. This concludes the main mechanisms: slower digestion, more gradual absorption, interaction with bile acids, bacterial fermentation, and increased satiety. From here, the next logical step is the intestine, where benefits, limitations, and individual differences become especially evident.
The intestine and tolerability: real benefits, practical limits, and individual differences
In brief: Fiber supports intestinal health, but not everyone responds in the same way. Fiber type, dose, hydration, and individual sensitivity determine real-world benefits, discomfort, and tolerability.
With this foundation in place, the first topic to explore in more depth is the gut microbiota, one of the most studied links between fiber and digestive function.
The intestine is the first place where the effects of dietary fiber become noticeable in daily life, but it is also the setting in which the limits of oversimplification become most apparent. On the one hand, fiber is often associated with improvements in bowel regularity, stool consistency, and interaction with the gut microbiota. On the other hand, individual responses can differ widely depending on dose, speed of introduction, hydration status, visceral sensitivity, and the presence of functional disorders such as irritable bowel syndrome, also referred to by the acronym IBS, a condition characterized by recurrent abdominal pain associated with changes in bowel habits [8][10]. This means the usefulness of fiber should never be interpreted as uniform. A type of fiber that improves bowel function and reduces constipation in one person may, in another, temporarily increase abdominal bloating, gas, and discomfort, especially if intake is increased too quickly. The evidence shows that fiber supplementation can improve bowel movement frequency and stool consistency in chronic constipation, but it may also increase subjective symptoms in the early stages or in more sensitive individuals [8]. In this context, talking about fiber also means talking about intestinal adaptation, gradual introduction, and personalization. Available data also show that the relationship between fiber and the intestine is bidirectional: fiber changes the intestinal environment, but the intestinal environment also shapes the response to fiber. Microbiota composition, intestinal motility, habitual intake of plant foods, and general health status substantially influence the practical outcome of increasing fiber intake. For this reason, it is useful to keep a few principles in mind:
- Intestinal benefit depends on the type of fiber, not just the total amount.
- The dose should be increased gradually, especially when the starting point is very low.
- Hydration remains important because many fibers require water to exert their effects.
- Initial bloating does not always mean true intolerance.
- In irritable bowel syndrome, the choice of fiber often matters more than the absolute amount.
Fiber and the gut microbiota
Dietary fiber is one of the main substrate sources for the gut microbiota, meaning the community of microorganisms that live in the colon and participate in fermentation processes, metabolite production, and maintenance of the intestinal environment. A fiber-rich diet, especially when it includes a variety of sources, tends to support greater microbial diversity, a feature often considered a marker of intestinal balance, although it should not be interpreted simplistically. Meta-analyses show that interventions based on increased fiber intake can raise the abundance of certain bacterial groups, including Bifidobacterium and Lactobacillus, and stimulate the production of SCFAs, the short-chain fatty acids derived from fermentation [9][10]. However, the available data also show marked individual variability. Baseline microbiota composition, habitual diet, medication use, physical activity level, and other environmental variables influence how fiber is metabolized and what type of response can be observed. For this reason, it is inaccurate to say that fiber “improves the microbiota” in a uniform and standardized way. More accurately, it provides a substrate that may support a more active and diverse intestinal environment, but with results that differ from person to person [9]. This clarification matters because it helps explain that intestinal benefit does not coincide with an immediate and identical change in all individuals. When improvement occurs, it tends to depend more on consistency and variety in fiber sources than on occasional one-off increases. From here, the discussion naturally moves to the most classic and concrete topic: the relationship between fiber and constipation.
Fiber and constipation
Constipation is one of the contexts in which fiber is used most frequently, but even here it is necessary to avoid the idea that “more fiber” always means “more benefit.” Fiber may help mainly through two mechanisms: it increases stool bulk and, in some cases, improves stool consistency by retaining water. Systematic reviews indicate that fiber supplementation can increase bowel movement frequency and improve stool consistency in individuals with chronic constipation, but they also show that not all fibers are equally effective and that the effect varies depending on the cause of constipation and individual tolerance [8]. Increasing intake too quickly may worsen symptoms, because the intestine needs time to adapt to a greater amount of fermentable material or fecal bulk. For this reason, the most effective nutritional strategies involve a gradualincrease combined with adequate hydration, meaning sufficient fluid intake to allow fiber to fully express its potential effect on stool consistency. In addition, not all forms of constipation depend primarily on a low-fiber diet, since sedentary behavior, medications, reduced intestinal motility, and functional disorders can all change the picture. Fiber, then, is a useful tool but not a universal one. Its effectiveness depends on the person, the type of symptom, and the way it is introduced. With that clarified, it is worth taking a closer look at stool consistency, a practical but often overlooked and clinically important indicator.
Fiber and stool consistency
In addition to influencing bowel movement frequency, dietary fiber also affects stool consistency, meaning the structure of stool in terms of firmness, softness, and ease of passage. This effect is especially relevant because regular bowel habits do not depend only on how often a person has a bowel movement, but also on stool quality and the comfort with which evacuation occurs. Some fibers, especially those able to absorb water and form gels, may help make stools more formed and regular, while others have a more noticeable effect on increasing bulk [8]. This aspect is useful not only in constipation, but also in conditions in which stools tend to be poorly formed, even without necessarily indicating pathological diarrhea. Still, it is important to avoid excessive generalization, because fiber is not a universal treatment for all bowel habit alterations and its use must always be interpreted within the clinical context. Available evidence supports the idea that the type of fiber makes a difference and that benefit depends on the ability to choose the form best suited to the individual [8][10]. Understanding the relationship between fiber and stool consistency helps avoid the mistake of evaluating fiber only in quantitative terms. In practice, what matters is not only how much fiber is introduced, but which fiber and with what degree of tolerability. This leads naturally to a very common issue in practice: abdominal bloating.
Fiber and abdominal bloating
Abdominal bloating is one of the most common effects of increasing fiber intake, and in most cases it is related to bacterial fermentation and gas production in the colon. Fermentable fibers, precisely because they are metabolized by the microbiota, can transiently increase the production of intestinal gas, especially when they are introduced quickly in people starting from a very low intake. This phenomenon does not automatically imply true intolerance, but often represents a phase of physiological adaptation [10]. Evidence indicates that many early symptoms tend to lessen over time as the microbiota adapts to the new substrate supply and the intestine develops better functional tolerance [10]. For this reason, the most effective strategy is usually not to eliminate fiber immediately at the first episode of bloating, but to slow the rate of increase, choose more tolerable sources, and distribute the daily intake more evenly across the day. Naturally, in individuals with marked intestinal sensitivity or persistent symptoms, evaluation must be more cautious. The key point is that bloating should not be interpreted in a binary way as either a “sign of benefit” or a “sign of harm,” but as a response that must be read within the individual context. This is especially important when moving into the territory of irritable bowel syndrome, which requires greater personalization.
Fiber and irritable bowel syndrome
In irritable bowel syndrome, or IBS, the relationship with dietary fiber becomes more complex, because the same fiber that improves bowel habits in one person may increase pain, bloating, and abdominal discomfort in another. This happens because IBS is characterized by greater visceral sensitivity and altered regulation of intestinal motility, conditions that make the patient more reactive to changes in intestinal contents and gas production. In this setting, the choice of fiber often matters more than the total amount. Highly fermentable fibers may be poorly tolerated by some sensitive individuals, whereas less fermentable fibers or fibers with gel-forming properties may be more manageable from a symptom perspective. The evidence supports the idea that there is no universal answer as to which fibers are best for all people with IBS, but that a personalized approach is needed, based on symptoms, tolerance, and method of introduction [8][10]. Here too, gradual introduction remains decisive, because a sudden increase may worsen symptoms regardless of the type of fiber selected. This makes it clear that fiber should not be demonized in irritable bowel syndrome, but neither should it be proposed in a standardized way. Its use requires closer clinical observation, greater attention to detail, and fewer automatic assumptions. Once this is understood, the final topic in this section can be addressed: the relationship between fiber and intestinal inflammation.
Fiber and intestinal inflammation
The relationship between dietary fiber and intestinal inflammation is a topic of growing interest, but it requires particularly cautious communication. From a biological standpoint, fiber fermentation and SCFA production, especially butyrate, suggest a possible contribution to maintaining intestinal barrier integrity and a more favorable mucosal environment. Butyrate, in fact, is a primary energy source for colonic epithelial cells and is associated with signals involved in the local regulation of intestinal balance [11]. However, clinical evidence does not allow fiber to be credited with a uniform or direct therapeutic effect on intestinal inflammation in all contexts. Results vary depending on the type of fiber, the overall diet, microbiota status, and the baseline condition of the intestine. For this reason, it is more accurate to say that fiber may contribute to a more balanced intestinal environment rather than present it as a specific tool for controlling inflammation [10][11]. In this context, fiber once again emerges as a nutritional factor that should be placed within a broader view of intestinal health, where dietary structure, tolerability, and personalization all matter. This concludes the section devoted to the intestine and leads naturally to the next topic: the role of fiber in prevention and cardiometabolic health.
Fiber, prevention, and cardiometabolic health
In brief: Fiber contributes to cardiometabolic prevention because it improves diet quality and acts on glycemia, lipids, satiety, and cardiovascular risk. Its value emerges most clearly when it is part of a minimally refined dietary pattern.
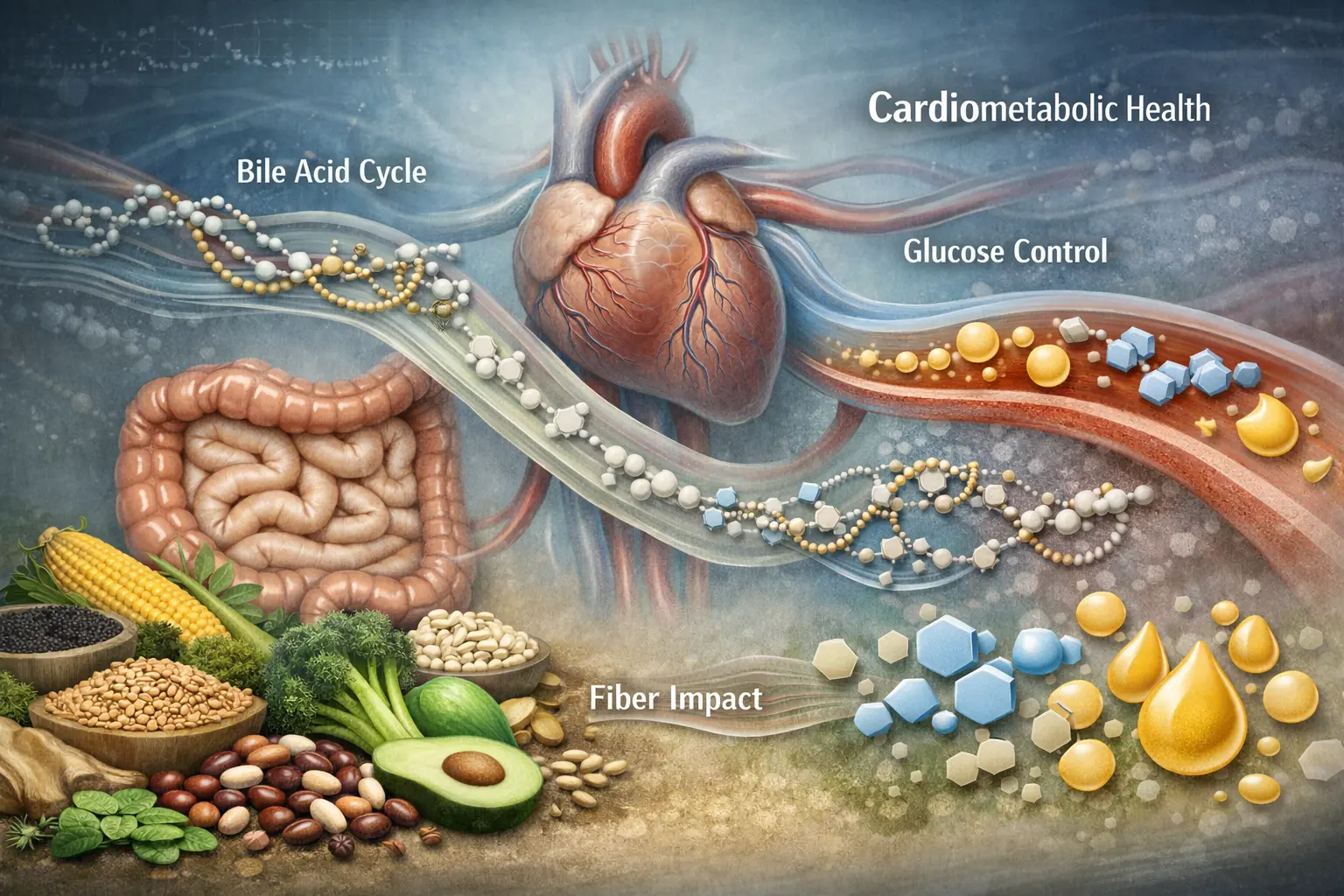
Interest in dietary fiber extends far beyond intestinal function and increasingly concerns cardiometabolic health, meaning the set of factors that connect metabolism, the cardiovascular system, and chronic disease risk. This framework includes altered glycemia, dyslipidemia, excess visceral fat, increased blood pressure, and worsening overall diet quality. Epidemiological evidence and meta-analyses consistently show that a higher fiber intake is associated with a lower risk of cardiovascular disease, type 2 diabetes, and all-cause mortality, but these findings must be interpreted rigorously, because fiber acts within an overall dietary context and not as an isolated element [2][14][17]. From a physiological perspective, fiber may modulate the rate of glucose absorption, influence bile acid and cholesterol metabolism, support satiety, and improve the structural quality of the diet. In other words, its contribution to prevention does not depend on a single mechanism, but on a set of coherent effects that converge toward better metabolic quality of the meal and of the diet as a whole. Available data show that this multifactorial action is precisely what makes fiber such a useful indicator of carbohydrate quality and, more broadly, of dietary pattern quality [3][17]. Still, miracle language must be avoided. Fiber does not “protect against everything,” it does not replace medical therapy, and it does not act on its own in the absence of a coherent diet. Its real value emerges when it is considered part of a dietary pattern rich in minimally refined plant foods, meaning foods that preserve more of the integrity of the original matrix and tend to have a more favorable metabolic impact. To navigate cardiometabolic prevention, a few essential points are worth keeping in mind:
- Fiber influences glycemia and insulin mainly by improving meal quality.
- It may contribute to improving the lipid profile, especially LDL cholesterol.
- It promotes greater satiety and better management of energy intake.
- It is associated with a lower risk of chronic disease within higher-quality dietary patterns.
- Its effect becomes more meaningful when it replaces refined and ultra-processed foods.
Fiber and type 2 diabetes
In the context of type 2 diabetes, dietary fiber plays a particularly important role because it helps improve carbohydrate quality and make the postprandial glycemic response more gradual. Meta-analyses indicate that higher intakes of fiber and whole grains are associated with better glycemic control, with reductions in HbA1c, meaning glycated hemoglobin that reflects average blood glucose levels over time, and fasting glucose in people with diabetes [3][6]. In addition, prospective studies show a dose-response relationship between fiber intake and lower risk of developing type 2 diabetes [15]. This effect depends on several factors acting together: slower glucose absorption, possible improvement in insulin sensitivity, greater satiety, and better overall diet quality. The evidence indicates that the benefit is especially evident when fiber comes from whole foods and legumes, meaning sources that change meal structure and not just the numeric fiber content [3]. It is therefore inaccurate to reduce the issue to the use of a single supplement or isolated fiber as a stand-alone strategy. Fiber does not replace therapy, but it is a coherent part of a broader nutritional strategy based on meal quality and consistency over time. This naturally leads to a broader but closely related clinical picture: metabolic syndrome.
Fiber and metabolic syndrome
Metabolic syndrome is a cluster of risk factors that includes abdominal obesity, altered glycemia, elevated triglycerides, reduced HDL cholesterol, and high blood pressure. In this context, dietary fiber can influence several parameters through indirect but coherent mechanisms: it improves carbohydrate quality, promotes greater satiety, may contribute to a better lipid profile, and helps reduce the overall energy density of the diet [17]. Evidence shows that a higher fiber intake is associated with a more favorable metabolic setting, but it is essential to clarify that fiber does not “cure” metabolic syndrome as if it were an isolated treatment. Its effect emerges when it is part of a dietary pattern richer in plant foods, lower in refined products, and better able to support sustainable energy balance over time. In this context, fiber-induced satiety and the slower rate at which some meals raise blood glucose are two particularly important elements [3][17]. The usefulness of fiber, then, lies in modifying some of the determinants of metabolic syndrome rather than providing an autonomous and direct effect. This interpretation also helps explain the more modest but still studied link between fiber and blood pressure.
Fiber and blood pressure
The relationship between dietary fiber and blood pressure is less intuitive than its relationship with glycemia and cholesterol, but it emerges in several evidence syntheses. Meta-analyses indicate that fiber intake, especially viscous fiber intake, may be associated with a modest reduction in blood pressure, although the size of the effect is generally limited and not always attributable exclusively to fiber [12][13]. This is because fiber-rich diets also tend to provide more potassium, magnesium, water, and plant-derived bioactive compounds, which in turn contribute to vascular health. The evidence therefore points to a favorable picture, but it does not justify presenting fiber as an isolated factor in blood pressure control. More accurately, higher fiber intake should be considered part of an overall dietary pattern better suited to supporting cardiovascular function, especially when it involves replacing refined products with less processed plant foods [4][12]. This once again reinforces the idea that the interest of fiber lies in its place within a coherent context. Once this is clear, it becomes possible to look at the broader and more robust topic: the association between fiber and overall cardiovascular risk.
Fiber and cardiovascular risk
Among the strongest areas in the literature, the association between dietary fiber and cardiovascular risk is supported by numerous meta-analyses and prospective studies. Evidence shows that higher fiber consumption is associated with a significant reduction in the risk of cardiovascular events and related mortality, especially when fiber comes from a diet rich in plant foods and whole grains [2][18]. This effect is probably mediated by a combination of factors: improved LDL cholesterol, better glycemic control, greater satiety, and better diet quality. Large observational studies, such as those conducted in the EPIC cohort, the European Prospective Investigation into Cancer and Nutrition, also show that higher consumption of plant foods and fiber is associated with a lower risk of ischemic heart disease [18]. It is important to emphasize that these are strong and consistent associations, not automatic individual guarantees. Fiber is one component of a protective dietary pattern, not an autonomous form of protection independent of the rest of the lifestyle. This balanced reading makes it possible to maintain both scientific rigor and practical usefulness. The next step, equally relevant in everyday perception, concerns the relationship between fiber and body weight control.
Fiber and weight control
Dietary fiber may contribute to body weight control mainly through indirect effects. Fiber-rich foods tend to have lower energy density, require more chewing, and increase satiety, creating a context that may facilitate better spontaneous regulation of calorie intake. Meta-analyses indicate that viscous fiber intake may be associated with modest reductions in body weight, BMI, meaning body mass index, and waist circumference, even in the absence of intentional calorie restriction [7][19]. However, these effects should not be overstated. Fiber is not a stand-alone solution for weight loss, nor is it a substitute for an overall dietary strategy. Its main value lies in its ability to improve diet quality, support satiety, and make a structurally favorable eating pattern more sustainable over the long term [7]. In other words, fiber helps more as a support for managing eating behavior than as an isolated weight-loss tool. This perspective helps avoid exaggerated promises and prepares the ground for the final subtopic in this section: the relationship between fiber and the colorectum.
Fiber and Colorectal Cancer Risk
The relationship between dietary fiber and colorectal cancer is one of the most studied in the nutrition literature. Meta-analyses indicate that higher fiber intake, particularly from whole grains, is associated with a lower risk of colorectal cancer [1]. Proposed mechanisms include increased fecal bulk, reduced intestinal transit time, and the production of SCFAs such as butyrate, which contributes to maintaining a more favorable intestinal environment [1][11]. These effects may reduce the contact time between the intestinal mucosa and potentially harmful substances and support a more balanced colonic physiology. However, even here it is essential to remember that we are talking about risk reduction, not absolute protection. Cancer risk is multifactorial and depends on a combination of genetics, lifestyle habits, dietary composition, physical activity, and other environmental factors. The evidence therefore indicates a consistent and biologically plausible association, but it calls for restrained communication. This concludes the overview of cardiometabolic prevention and naturally opens the discussion of different life stages and more delicate clinical contexts.
Fiber across the life course and in more delicate contexts
In brief: Fiber remains useful at every age, but its practical meaning changes according to life stage, intestinal tolerance, and clinical goals. For this reason, adaptation, gradual introduction, and common sense are essential.
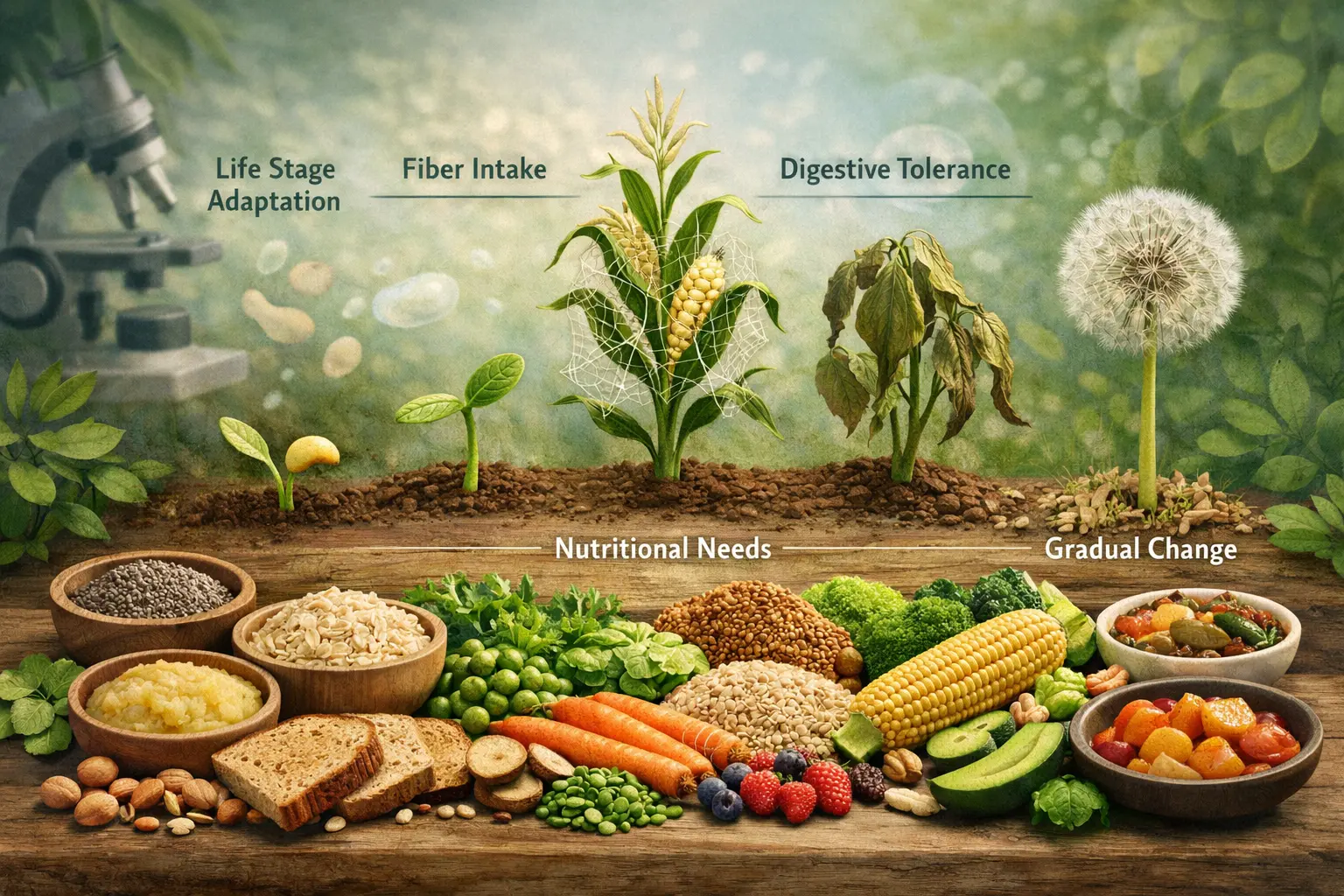
Dietary fiber does not have the same practical meaning at every stage of life, because requirements, tolerability, clinical goals, and the ability to introduce fiber-rich foods change with age, physiological status, and the person’s metabolic condition. International guidelines provide general thresholds that are useful as reference points, but their real-world application must be adapted to individual needs, avoiding both generalizations and the idea that the same nutritional plan works identically for everyone. In adults, about 25 grams per day is a widely used minimum reference threshold, but this value should always be interpreted in relation to intestinal tolerance, diet quality, and clinical context [3][17]. In some specific situations, such as pregnancy, childhood, older age, menopause, and metabolic conditions such as prediabetes, fiber may play a particularly useful role, but it requires more careful methods of introduction. The same amount that may be easily tolerated by a young adult accustomed to a plant-based diet could be much harder to manage in an older person with poor fluid intake, or in someone starting from a very low-fiber diet and already experiencing intestinal symptoms. Available data suggest that fiber should always be integrated into a broader practical assessment that also considers hydration, appetite, intestinal motility, and overall diet quality [8][15]. This approach helps avoid both excessive caution, which leads to underestimating the contribution of fiber, and the opposite automatism, which pushes toward rapidly increasing intake without taking the person into account. To navigate this section more effectively, it is useful to keep a few basic principles in mind:
- Tolerance to fiber changes with age, intestinal symptoms, and dietary habits.
- In pregnancy and older age, gradual introduction is especially important.
- In children, building healthy habits matters more than an abstract number of grams.
- In prediabetes, the value of fiber depends mainly on improving carbohydrate quality.
- In the presence of intestinal symptoms, intake should be increased gradually and personalized.
Fiber During Pregnancy
During pregnancy, dietary fiber can be especially helpful because it helps counteract constipation, which tends to occur more frequently due to hormonal changes, altered intestinal motility, and, in some cases, reduced physical activity. Adequate fiber intake also helps improve overall diet quality, increase satiety, and support a better distribution of carbohydrates throughout the day. However, intake should be increased gradually, because a rise that is too rapid can worsen bloating, gas, and discomfort [8]. The most useful strategy is usually one based on naturally fiber-rich foods such as legumes, whole fruit, vegetables, and less refined grains, combined with good hydration, since water remains essential for the proper function of many types of fiber. In this context, the evidence indicates that fiber should be considered part of a balanced dietary pattern, not an isolated remedy or a mechanical intervention [3]. This makes it possible to keep the discussion practical, without attributing properties to fiber that are not supported by the literature. Once the context of pregnancy has been clarified, the next step is to consider pediatric age, where the issue of fiber should be viewed mainly from an educational perspective and in terms of habit formation.
Fiber in Children and Adolescents
In children and adolescents, dietary fiber plays an important role because it helps build healthy eating habits and normalize the presence of plant foods in the daily diet. In this age group, the goal should not be the obsessive pursuit of a precise number, but the regular and sustainable introduction of fruit, vegetables, legumes, and less refined grains. An overly technical approach risks turning an educational topic into a source of rigidity or food refusal. From a practical standpoint, fiber can contribute to bowel regularity and meal quality, but it is essential that it be introduced within a balanced diet and not as a forced addition. Tolerance remains important, because even in younger individuals a fiber increase that is too rapid can promote bloating or poor acceptance. The evidence suggests that the value of fiber during growth lies mainly in promoting a varied diet based on structurally simple, minimally refined foods [3]. This perspective reinforces the idea that fiber should be viewed as a component of dietary quality rather than an abstract target. As age advances, however, practical limits change, and the role of hydration becomes even more decisive, as it does in older adults.
Fiber in Older Adults
In older adults, dietary fiber can contribute significantly to bowel regularity, especially in the presence of a sedentary lifestyle, reduced motility, and frequent use of medications that may slow intestinal transit. However, precisely at this stage of life, increasing fiber requires particular caution, because high intake without adequate hydration can worsen constipation rather than improve it. In addition, factors such as dentition, poor appetite, difficulty preparing meals, and a preference for softer or more refined foods may reduce spontaneous intake of natural fiber sources [8]. For this reason, the most useful strategy is almost always gradual and personalized. What matters is not only the total amount, but also how easily fiber-rich foods can be eaten and tolerated. Well-prepared legumes, fruit, cooked vegetables, and less refined grains can be practical solutions, provided that the overall context is sustainable. The evidence indicates that the effectiveness of fiber in older adults depends far more on the balance between dose, water, and tolerability than on rigid numerical targets [8]. This makes it clear that the approach to fiber in older adults must be concrete and realistic, and it opens the discussion on menopause, a phase in which the meaning of fiber is linked mainly to the metabolic context.
Fiber in Menopause
During menopause, dietary fiber can help improve overall diet quality and support body weight control, which often becomes more delicate at this stage because of metabolic changes, shifts in body composition, and reduced energy expenditure. A diet rich in plant foods and minimally refined foods promotes satiety, improves the nutrient density of the meal, and may make long-term energy balance easier to manage [7][17]. It is important to avoid inappropriate claims, because fiber does not have a direct hormonal effect and does not by itself “correct” the typical changes of menopause. Its contribution is indirect but meaningful, because it helps improve carbohydrate quality, appetite regulation, and the overall dietary profile. In this context, the value of fiber emerges mainly as a support tool within a coherent and sustainable dietary pattern, rather than as an isolated intervention. This interpretation sets up the next topic well, where the relationship between fiber and carbohydrate quality becomes even more central: prediabetes.
Fiber for People with Prediabetes
In prediabetes, that is, the stage in which blood glucose regulation is impaired but does not yet meet the criteria for overt diabetes, dietary fiber is a particularly useful nutritional tool because it improves carbohydrate quality and makes the glycemic response to meals more gradual. The evidence indicates that high-fiber diets are associated with a lower risk of progression to type 2 diabetes, especially when the fiber comes from natural foods and replaces refined sources [3][15]. The key point is not the isolated addition of a supplement, but the progressive replacement of low-structure foods with legumes, whole grains, whole fruit, and vegetables, which change the entire dynamics of the meal. Available data show that the benefit depends as much on the dietary context as on the amount of fiber achieved. For this reason, in prediabetes fiber should be considered a practical marker of carbohydrate quality rather than an accessory corrective measure. This leads to the final subtopic of the section, namely the situations in which increasing fiber requires greater caution.
When to Increase Fiber with Caution
Increasing dietary fiber requires caution especially when a person starts from a very low intake or has intestinal symptoms such as bloating, pain, irregular bowel habits, or marked digestive sensitivity. In these cases, a sudden increase can worsen discomfort and make the intervention harder to maintain over time. The evidence indicates that a gradual rise in intake is the most effective strategy for helping the intestine and the microbiota adapt, reducing the risk of adverse effects [8][10]. Caution is also important in people with IBS, in those who drink little, in older adults, and in those who use fiber supplements without an adequate understanding of dose and tolerability. The most solid practical rule is to increase one source at a time, observe the body’s response, and maintain fluid intake consistent with the amount of fiber introduced. This approach does not reduce the value of fiber; it makes it more realistic and more sustainable. This completes the overview of the different life stages and the more delicate contexts, opening the way to the next step: understanding where to find fiber and how to navigate among foods, packaged products, and supplementation.
Where to Find Fiber and How to Navigate Different Sources and Forms
In brief: Fiber is found mainly in minimally refined plant foods, but not all sources carry the same practical meaning. What matters is the food matrix, not just the number printed on the label.

Knowing that dietary fiber is beneficial is not enough unless one understands where to obtain it and how to choose among natural food sources, packaged products, and supplements. This is one of the most delicate steps in translating scientific evidence into everyday practice, because the most common risk is reducing the issue to a simple gram count, losing sight of the fact that fiber acts within a food matrix, that is, within a food structure that includes water, micronutrients, bioactive compounds, texture, and degree of processing. The evidence shows that diets rich in fiber from natural sources are associated with more favorable health outcomes than patterns in which fiber is introduced mainly as an isolated addition [3][17]. This does not mean that supplements have no role, but it does imply that the first goal should almost always be to increase fiber through legumes, whole grains, vegetables, whole fruit, seeds, and nuts, that is, through foods that simultaneously improve meal structure, satiety, and overall diet quality. A packaged product may list an appreciable fiber content on the label and still be metabolically poor in quality if it is part of a highly refined or ultraprocessed formulation. Conversely, a simple, minimally refined food may provide a fiber amount that is not exceptional per serving, yet within a much more favorable nutritional context [18]. Available data suggest that fiber should be interpreted not only as a quantity, but as a signal of the quality of the food and the diet as a whole. To navigate practically among different sources and forms, it is useful to keep a few basic principles in mind:
- Natural sources remain the main reference point for increasing fiber.
- Legumes are especially strategic because they combine fiber with good overall meal quality.
- The food matrix matters as much as, and often more than, the number of grams.
- Supplements can be useful in targeted contexts, but they do not replace a well-structured diet.
- Not all fibers have the same use, because their properties and tolerability differ.
The Foods Richest in Fiber
The main sources of dietary fiber are legumes, whole grains, fruit, vegetables, seeds, and nuts, but their real contribution depends not only on the content per 100 grams, but also on the amount actually consumed and how often they appear in the diet. Legumes are one of the most efficient sources because they combine fiber, plant protein, and a generally more favorable carbohydrate structure. Whole grains, by contrast, have a major impact when they replace refined versions of bread, pasta, rice, and breakfast cereals, thereby improving the overall quality of the meal [3][18]. Fruit and vegetables, although in many cases less concentrated in fiber than legumes, become highly relevant when consumed regularly and in adequate portions. They also bring water, micronutrients, and bioactive compounds that are part of the food matrix and contribute to their overall value. The evidence shows that regular consumption of fiber-rich plant foods is associated with a reduced risk of chronic diseases, including ischemic heart disease [18]. This suggests that there is no single “best” food in absolute terms, but rather a combination of sources that, added together over the course of the day, builds an effective and sustainable intake. From this comes a very common question: is it better to focus mainly on legumes or on whole grains?
Legumes or Whole Grains?
The comparison between legumes and whole grains is common, but in reality these foods are complementary rather than alternative. Legumes provide large amounts of dietary fiber per serving and are one of the most effective strategies for increasing total intake quickly yet in a structured way. Whole grains, on the other hand, have the advantage of improving the most routine meals, because they easily replace refined products such as bread, pasta, or white rice, thereby enhancing everyday diet quality [3]. The evidence shows that both categories contribute significantly to reducing the risk of chronic disease, but through partly different mechanisms. Legumes have a strong impact on satiety and the carbohydrate load of the meal, while whole grains more stably improve the quality of the starchy base of the diet. For this reason, from a practical standpoint, combining legumes and whole grains is often the most effective and sustainable strategy, because it increases fiber without depending on a single food category [18]. This helps shift the focus away from the search for the “perfect food” and toward building a more coherent diet. Alongside legumes and grains, however, the contribution of fruit and vegetables remains essential and deserves specific attention.
Fiber-Rich Fruit and Vegetables
Fruit and vegetables contribute significantly to dietary fiber intake, but their impact depends on the amount consumed, the variety, and the way they are incorporated into meals. Whole fruit is generally preferable to juice because it preserves the original fibrous structure and slows sugar absorption, while vegetables are especially useful when they are not treated as a marginal side dish, but as a stable and substantial component of the meal. Some foods, such as fibrous vegetables, fresh legumes, and less watery fruits, can make a more relevant contribution to the daily total [18]. The evidence indicates that high fruit and vegetable consumption is associated with better health outcomes also thanks to the contribution of fiber, but the benefit does not depend only on the numerical fiber content. It also matters that these foods improve overall diet quality, nutrient density, satiety, and the variety of substrates available to the microbiota [16][18]. For this reason, the most effective strategy remains increasing variety and frequency rather than focusing obsessively on a single very high-fiber food. Once the role of natural food is clear, it becomes inevitable to address the comparison with fiber supplements, which are often perceived as easier shortcuts.
Food or Fiber Supplements?
Fiber supplements can have a role in some specific situations, but in most cases they are not the first choice. The evidence indicates that fiber derived from natural foods is associated with broader benefits, because it comes together with a complex food matrix that includes micronutrients, water, structure, and bioactive compounds [3][17]. A supplement may provide a fiber with targeted properties, for example a viscous fiber useful for glycemic or lipid control, but it does not replace the overall effect of a diet rich in minimally refined plant foods. This means that supplementation should be considered a possible complementary support, not an alternative to building a good dietary foundation. Supplements may be useful when dietary intake remains inadequate, when a person has practical difficulty reaching appropriate amounts, or when a specific property is being sought, but their use should remain contextualized and cautious [6][8]. The strongest practical hierarchy therefore remains this: first improve the food, then, if needed, consider targeted supplementation. Once this point is clear, it becomes necessary to address an increasingly important distinction: that between a food naturally rich in fiber and an ultraprocessed product with added fiber.
Fresh Food vs Ultraprocessed Foods
An ultraprocessed food with added fiber is not metabolically or nutritionally equivalent to a food naturally rich in dietary fiber. The main difference lies in the food matrix, meaning that in fresh or minimally processed food, fiber is embedded in a complex plant structure that also includes water, vitamins, minerals, polyphenols, and lower energy density. In ultraprocessed products, fiber may be added within a less favorable context characterized by refined starches, sugars, low-quality fats, and high palatability [17]. The evidence suggests that the overall quality of the diet matters more than the single nutrient reported on the label, and that the number of grams of fiber alone is therefore not enough to define the value of a food [17][18]. This does not mean that every enriched product is useless, but it does imply that it cannot be judged solely on the basis of declared fiber. In practice, added fiber may improve a product, but it does not automatically transform a highly refined food into something equivalent to legumes, vegetables, or whole grains. At this point, it is worth looking at some specific fibers that receive a lot of attention, such as inulin, psyllium, and beta-glucans, because they help illustrate how properties and uses can differ.
Inulin, Psyllium, and Beta-Glucans
Some specific fibers, such as inulin, psyllium, and beta-glucans, are often mentioned because they have fairly recognizable functional properties. Inulin is a highly fermentable fiber and is often discussed for its relationship with the gut microbiota. Psyllium is known for its ability to absorb water and form gels, making it useful for stool consistency and, in some contexts, for glycemic and lipid profile. Beta-glucans, found especially in oats and barley, are associated with favorable effects on LDL cholesterol and glycemic response, partly thanks to their viscosity [5][6]. Meta-analyses show that fibers with viscous properties can have significant effects on glycemia and lipids, but these effects always depend on dose, consistency of use, and the dietary context in which they are introduced [5][6]. There is therefore no single fiber that is “best” in absolute terms, but rather different options with different properties, which may be more or less suitable depending on the goal and individual tolerability. This distinction closes the section devoted to the sources and forms of fiber and sets up the next step, which concerns the most practical way to increase intake sustainably.
How to Increase Fiber in a Practical, Gradual, and Sustainable Way
In brief: Increasing fiber works only if the change is progressive, realistic, and well distributed throughout the day. Graduality, hydration, and source selection matter more than the rush to reach a number.

Increasing dietary fiber intake is not a mechanical operation, but a process that requires adaptation, consistency, and a good understanding of one’s starting habits. Many people run into difficulty not because the strategy is wrong, but because the change is implemented too quickly or in an unsustainable way, often with sudden increases in legumes, whole grains, or supplements without giving the intestine enough time to adapt. The evidence indicates that a progressive increase allows the gut microbiota and digestive function to respond more favorably, reducing the risk of bloating and discomfort [8][10]. Another decisive point is hydration, because many fibers absorb water and function better when fluid intake is adequate. Without enough water, the benefit for intestinal transit may be reduced and, in some situations, constipation may even worsen. At the same time, it should be remembered that increasing fiber does not mean randomly adding a few “healthy” foods, but rather distributing sources better throughout the day and progressively replacing refined foods with options that have more structure [3][8]. Available data show that the most effective change is almost always the one that improves the overall dietary profile without creating unmanageable disruptions in daily routine. For this reason, it is useful to keep a few key practical principles in mind:
- Increasing one fiber source at a time is often more effective than changing everything at once.
- Distributing fiber throughout the day improves tolerability.
- Drinking enough water is essential when fiber intake increases.
- Reading the nutrition facts panel is useful, but it should be combined with an evaluation of the ingredients.
- Slower changes are often the ones that last longest.
How to Increase Fiber Without Bloating
Abdominal bloating is one of the main obstacles when trying to increase dietary fiber, but in most cases it depends more on the speed of change than on fiber itself. When a person suddenly shifts from a low-fiber diet to one very rich in legumes, fibrous vegetables, or whole grains, the gut microbiota receives a much larger amount of fermentable substrate and may increase gas production rapidly. The evidence indicates that many of these symptoms tend to decrease over time, provided that introduction is progressive and the amount is distributed more evenly throughout the day [10]. From a practical standpoint, the most useful approach is to increase only one food category at a time, observe the intestinal response, and keep that change consistent for a few days before adding another. Source selection also matters: some fibers are more tolerable than others, and the way food is prepared can make a concrete difference. The principle is not to give up fiber at the first sign of discomfort, but to make adaptation more manageable and more consistent with the person’s sensitivity. This logic leads naturally into the next subtopic, which concerns the concrete organization of a more fiber-rich eating day.
Example of a High-Fiber Menu
A diet rich in dietary fiber does not require exotic foods or especially complex meal plans, but rather a better distribution of sources throughout the day. A typical day might begin with a breakfast that includes whole grains and whole fruit, continue with a lunch based on legumes, vegetables, and a portion of less refined grains, and end with a dinner in which vegetables, a whole-grain or semi-whole-grain starchy source, and a less refined meal structure help complete the daily balance. The goal is not to concentrate all fiber in a single meal, because that choice often worsens tolerability, but to distribute it in a way that improves both intestinal response and the metabolic quality of meals. Available data show that fiber intake works better and is more sustainable when placed within a coherent dietary pattern than when one chases individual foods perceived as “superior” [3][17]. This also helps avoid the mistake of using one single food as a total solution. After setting up the practical organization of meals, it becomes useful to understand how to read the labels of packaged foods without stopping at the number of grams of fiber alone.
How to Read Labels
Reading nutrition labels is a useful tool for evaluating the dietary fiber content of packaged foods, but it should never be used in isolation. The number of grams reported in the table is certainly informative, but it must be interpreted together with the ingredients, the degree of processing, and the product’s overall profile. A food may contain a decent amount of added fiber and still remain highly refined or ultraprocessed, with a less favorable metabolic impact than a simple food naturally rich in fiber [17]. For this reason, reading the label means asking not only “how much fiber is there,” but also “where does it come from,” “what ingredients accompany it,” and “what place does this product occupy within the diet.” The evidence indicates that the overall quality of the diet remains more important than the single nutrient listed on the package [17][18]. This approach helps people make more realistic choices and fewer choices driven by marketing. Once it is clear how to evaluate products, it is worth looking at the most common mistakes that get in the way of a good increase in fiber intake.
Common Mistakes with Fiber
The three most common mistakes when trying to increase dietary fiber are moving too fast, drinking too little, and relying on a single source believed to be the solution. A sudden increase can amplify bloating and intestinal discomfort, reducing adherence to the change within the first few days. Poor hydration limits the effectiveness of many fibers and can worsen constipation, while concentrating on a single food reduces variety and sustainability [8][10]. Another common mistake is ignoring individual tolerance, choosing highly fermentable sources or sources poorly suited to one’s intestinal sensitivity simply because they are perceived as “healthier.” The evidence indicates that a gradual, diversified, and personalized approach works better than drastic, standardized changes [8]. In this context, the quality of the strategy matters more than how quickly a certain number of grams is reached. From here, the discussion naturally moves to the specific role of water, which is a decisive companion to any increase in fiber.
Water and Fiber
Water is fundamental to the proper function of many dietary fibers, because various fibers absorb fluids, increase in volume, and help form softer, more regular stools precisely through their interaction with hydration. If fluid intake is insufficient, the benefit for intestinal transit is reduced and, in some cases, the situation may even worsen. This is especially true when supplemental fibers are introduced or when intake is rapidly increased from dry sources such as whole grains and seeds [8]. This does not mean that there is one identical amount of water suitable for everyone, but rather that hydration should increase in line with the amount of fiber introduced, the climate, physical activity, and the characteristics of the individual. The evidence and clinical practice converge in considering water an essential factor in making increased fiber useful and well tolerated [8]. This clarifies why talking about fiber without talking about fluids is always an incomplete simplification. Once this point is understood, one final practical question remains for this section: whether there is a better time of day to eat more fiber.
When to Eat More Fiber During the Day
Distributing dietary fiber throughout the day is generally preferable to concentrating it in a single meal, because a more even distribution tends to improve intestinal tolerability and promote a more stable metabolic response. Including fiber at breakfast, lunch, and dinner, with possibly small amounts in snacks as well, helps avoid excessive loads that could worsen bloating or discomfort, especially in more sensitive individuals [10]. In addition, a regular distribution of fiber improves the overall quality of meals and helps sustain satiety throughout the day, reducing the effect of meals that are very quick and lacking in structure. Available data suggest that the greatest benefit does not depend on a “magic” time of day, but on consistency and on integrating fiber into complete, minimally refined meals [3][19]. Besides being more physiological, this approach is also more feasible over the long term. This concludes the most practical part of the article and opens the final major section devoted to what science really shows, the limits of the evidence, and the most widespread myths.
What we really know: evidence, guidelines, and myths
In brief: Evidence on dietary fiber is consistently favorable, but it must be interpreted with rigor—without overstating its effects. Guidelines offer useful intake thresholds, while misconceptions tend to arise when fiber’s role is oversimplified.
When discussing dietary fiber, it is easy to fall into two opposite traps. On one side, fiber is reduced to a basic aid for bowel regularity; on the other, it is portrayed as a universal fix for metabolic and digestive issues. Both perspectives are misleading. The strongest evidence shows that higher fiber intake—particularly within diets rich in minimally refined plant-based foods—is associated with improved health outcomes, including lower risk of cardiovascular disease, type 2 diabetes, and all-cause mortality [2][14][17]. However, these findings do not justify treating fiber as a standalone or “miracle” component detached from the broader diet. Scientifically, this body of evidence is robust because it draws on converging results from prospective studies, systematic reviews, and meta-analyses. These consistently show associations and, in many cases, dose–response relationships. At the same time, important limitations remain: variability in fiber types studied, difficulty separating fiber from overall dietary patterns, and significant individual differences in intestinal and metabolic responses. For this reason, guidelines translate evidence into minimum intake targets and practical advice, while emphasizing carbohydrate quality and prioritizing natural, minimally processed foods [3][17]. To navigate the topic without oversimplifying, a few key principles are worth keeping in mind:
- Evidence overall supports fiber intake, but dietary context is critical.
- Fibers differ significantly in structure and function.
- Guidelines indicate minimum thresholds, not universal targets.
- The most reliable data concern fiber-rich dietary patterns, not occasional additions.
- Misconceptions often arise from oversimplifying fiber physiology.
What research shows
High-quality scientific syntheses consistently link higher dietary fiber intake with meaningful health benefits. Meta-analyses highlight a dose–response relationship between fiber consumption and reduced risk of chronic disease, with measurable effects beginning around 25–29 grams per day [3]. Large prospective studies also show associations between higher fiber intake and lower all-cause and cardiovascular mortality, reinforcing the role of fiber as a marker of overall diet quality [14][16]. Another key point is how fiber is consumed. The most consistent benefits are observed when fiber comes from whole, minimally refined foods rather than isolated supplements. This reinforces the concept that fiber operates within a food matrix—it does not act independently of the meal or dietary pattern. Within this context, fiber plays a consistent role in improving metabolic quality and supporting disease prevention. While this overall picture is clearly favorable, it is equally important to consider the limits of the available evidence.
Where the evidence falls short
Despite its consistency, research on dietary fiber has notable limitations. Much of the data comes from observational studies, which identify associations but cannot establish direct causality. Individuals with higher fiber intake often also engage in other healthy behaviors, such as being more physically active, consuming fewer ultra-processed foods, and maintaining better overall diet quality [17]. This overlap makes it difficult to isolate fiber’s independent effect. Clinical trials add further complexity. They vary widely in fiber type, dosage, duration, study populations, and measured outcomes. Umbrella reviews suggest that while fiber generally improves cardiometabolic risk factors, the magnitude of these effects is often moderate and varies across contexts [17]. In short, the evidence supports real benefits, but it calls for careful interpretation and measured communication. Recognizing these limitations does not diminish fiber’s importance—it clarifies its role. This naturally leads to the question of how official guidelines translate the evidence into practice.
Fiber in official guidelines
Official guidelines provide the most practical framework for applying scientific evidence on dietary fiber. The World Health Organization and other international bodies typically recommend a minimum intake of around 25 grams per day for adults. EFSA (European Food Safety Authority) considers this level adequate for supporting normal bowel function and guiding carbohydrate quality. Across Europe, recommendations generally fall between 25 and 35 grams per day, adjusted according to energy intake and individual needs [3]. However, quantity is only part of the picture. Guidelines consistently stress that fiber should come primarily from minimally refined plant-based foods. The observed benefits depend on the overall dietary pattern—not just the fiber content itself. In this sense, fiber serves as a practical indicator of diet quality, carbohydrate structure, and metabolic health [3][17]. This means that while numerical targets are useful, they should not overshadow the importance of food quality. Oversimplifying these recommendations often leads to persistent myths.
Common misconceptions about fiber
Dietary fiber is frequently misunderstood due to oversimplification. A common myth is that all fibers behave the same way. In reality, properties such as viscosity, fermentability, and solubility lead to very different physiological effects, both intestinal and metabolic [5][6]. Another widespread misconception is that increasing fiber intake is always beneficial. In practice, rapid increases can cause bloating and gastrointestinal discomfort, especially in individuals with IBS or heightened sensitivity [8][10]. It is also incorrect to assume that adding a single high-fiber food or supplement can compensate for an overall poor diet. Evidence shows that fiber works best when it is part of a consistent dietary pattern rich in minimally refined plant foods and lower in ultra-processed products [17]. In other words, fiber’s value must always be understood within the broader structure of meals and overall diet.
High-fiber vs low-fiber diets
Comparing high- and low-fiber diets highlights broader differences in dietary quality. High-fiber diets typically include more legumes, whole grains, fruits, and vegetables—foods that are naturally rich in minimally refined plant components. These patterns are associated with improved glycemic regulation, greater satiety, and a more favorable metabolic profile. By contrast, low-fiber diets often rely more heavily on refined and ultra-processed foods. This reduces dietary complexity and negatively affects carbohydrate quality [2][17]. Evidence consistently links lower fiber intake with increased risk of chronic diseases and poorer overall diet quality [2][14]. In this sense, fiber acts not only as a nutrient but also as a practical marker of how close a diet is to a more protective or less favorable pattern.
Is there a “best” type of fiber?
There is no universally “best” fiber. Its usefulness depends on the specific goal, individual tolerance, and clinical context. For constipation, fibers that increase stool bulk or improve stool consistency may be beneficial. For glycemic control, viscous fibers are often more relevant. For microbiota-related effects, fermentable fibers play a key role [5][6][8]. This means fiber selection should be personalized rather than based on rankings or trends. Such an approach avoids unrealistic expectations and helps explain why a widely promoted fiber may not produce the same effect in every individual.
Conclusions and editorial summary
Dietary fiber remains one of the most consistently studied components linked to metabolic, intestinal, and cardiovascular health. Its relevance stems from its multi-level physiological effects: it slows nutrient absorption, modulates glycemic and insulin responses, contributes to LDL cholesterol control, and supports gut microbiota regulation through metabolite production. Meta-analyses and systematic reviews consistently associate higher fiber intake with reduced risk of chronic disease and mortality. However, this relationship must be understood within its proper context. Fiber does not act in isolation; rather, it reflects broader dietary patterns characterized by higher consumption of minimally refined plant foods and lower intake of ultra-processed products. A central consideration is variability. Fibers differ in function, and individual responses depend on microbiota composition, metabolic status, dosage, and how fiber is introduced into the diet. This reinforces the need for a personalized, nuanced approach. From a practical standpoint, increasing fiber intake through natural food sources aligns with the strongest available evidence. This should be done gradually and sustainably. Ultimately, overall diet quality remains the key determinant, with fiber serving as a valuable indicator. In essence, fiber is not a standalone solution or universal intervention. It is a structural component of a balanced diet, whose impact depends on its integration with broader nutritional and lifestyle factors.
References
[1] Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies
[2] Dietary fibre intake and risk of cardiovascular disease: systematic review and meta-analysis
[3] Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses
[4] Dietary fibre in hypertension and cardiovascular disease management: systematic review and meta-analyses
[5] Galactomannans are the most effective soluble dietary fibers in type 2 diabetes: a systematic review and network meta-analysis
[6] Should Viscous Fiber Supplements Be Considered in Diabetes Control? Results From a Systematic Review and Meta-analysis of Randomized Controlled Trials
[7] Can dietary viscous fiber affect body weight independently of an energy-restrictive diet? A systematic review and meta-analysis of randomized controlled trials
[8] The Effect of Fiber Supplementation on Chronic Constipation in Adults: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
[9] Dietary fiber intervention on gut microbiota composition in healthy adults: a systematic review and meta-analysis
[10] Effects of Dietary Fibers on Short-Chain Fatty Acids and Gut Microbiota Composition in Healthy Adults: A Systematic Review
[11] From Dietary Fiber to Host Physiology: Short-Chain Fatty Acids as Key Bacterial Metabolites
[12] The effect of viscous soluble fiber on blood pressure: A systematic review and meta-analysis of randomized controlled trials
[13] Dietary Fiber and Blood Pressure: A Meta-analysis of Randomized Placebo-Controlled Trials
[14] Association Between Dietary Fiber and Lower Risk of All-Cause Mortality: A Meta-Analysis of Cohort Studies
[15] Dietary fiber intake and risk of type 2 diabetes: a dose-response analysis of prospective studies
[16] Associations between dietary fiber intake and mortality from all causes, cardiovascular disease and cancer: a prospective study
[17] Associations between dietary fiber intake and cardiovascular risk factors: An umbrella review of meta-analyses of randomized controlled trials
[18] Plant foods, dietary fibre and risk of ischaemic heart disease in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort
[19] Unravelling the Effects of Soluble Dietary Fibre Supplementation on Energy Intake and Perceived Satiety in Healthy Adults: Evidence from Systematic Review and Meta-Analysis of Randomised-Controlled Trials
[20] Prolonged Isolated Soluble Dietary Fibre Supplementation in Overweight and Obese Patients: A Systematic Review with Meta-Analysis of Randomised Controlled Trials
Editorial note
Artificial Intelligence was used solely as a tool to support editorial and documentary work. All content, interpretations, bibliographic citations and conclusions have been verified, reviewed and approved by the author, who assumes full scientific responsibility for them.
The manuscript was also subject to independent peer review prior to publication.
To ensure maximum transparency, the article's complete history — including the dates of submission, review, acceptance and publication, as well as information on the peer review process — is available on the dedicated Article History page.